Illinois has strengthened access to speech therapy for people recovering from brain injuries. On June 26, 2026, Gov. JB Pritzker signed SB 2899 into law as Public Act 104-0528. The measure amends the Illinois Insurance Code and Public Aid Code to require coverage of rehabilitative services for individuals under 19 with an early acquired speech-language disorder. It also directs Medicaid to cover rehabilitative stuttering therapies for those 21 and under. The insurance provisions take effect January 1, 2028.
The change matters for brain injury survivors, as rehabilitative speech therapy is often central to recovery. By mandating coverage of rehabilitative care, the law helps ensure that survivors have access to therapies designed to help them regain their ability to communicate.
As Senator Willie Preston (IL-16), the bill’s sponsor, said “young people [now] have access to the tools, support and treatment they need to find their voice and be heard.”
Extreme heat is a direct threat to the brain. When the body cannot shed heat fast enough, core temperature climbs and heat stroke can follow. This medical emergency leads to overheated blood damaged neurons and can result in cognitive impairment. People already living with a brain injury are especially vulnerable, as damaged temperature-regulating systems make it harder to cool down and easier to slip into confusion, seizures, or worsening symptoms.
Prevention, though, is straightforward and quite simple: hydrate constantly, rest in shade or air conditioning, avoid exertion during the hottest time of the day, and wear light clothing. Most importantly, treat dizziness, nausea, or confusion as warning signs and call 911 immediately when there is sudden confusion or a collapse.
Government response has been uneven. The Occupational Safety and Health Administration’s original Heat National Emphasis Program expired in April 2026 and was replaced by a revised, expanded federal program running through April 2031. H.R. 6213 and S. 4427 would prevent the Department of Labor from putting a national heat safety rule into action.
On July 21, 2026, the House Education and Workforce Committee advanced the Heat Workforce Standards Act in an 18-15 party-line vote to block OSHA from finalizing such a rule. Opposing it, Rep. Alma Adams (NC) challenged colleagues to “stack boxes on Independence Avenue for a few hours without water and without shade.” In support of the bill, Rep. Tim Walberg (MI) argued that it isn’t fair to impose a “one-size-fits-all” federal mandate across very different industries, climates, and workplace environments. Though all states have extreme temperature concerns, as can be attested in the Northeast right now, it is notable that the opposition comes from not only party lines, but also from regions of the country that often have heat waves.
Governor Josh Green signed Act 259 (HB 2021) on July 15, 2026, giving Hawaii its first comprehensive statewide e-bike framework. The law requires helmets for all riders under 18, bars anyone under 15 from operating an e-bike, and prohibits riders under 16 from using Class 2 or Class 3 models without adult supervision.
The measure grew out of an alarming rise in head trauma. Hawaii Department of Health data reported that e-bike injuries more than doubled between 2022 and 2025, from 106 to 244. Honolulu EMS also found that 81 percent of the e-bike patients that were treated wore no head protection. Honolulu-based Kapi’olani Medical Center’s trauma team reported that e-bike crashes recently became the leading cause of injury among the children it treated.
Green, previously an emergency physician, has been blunt about the stakes. “If they have a head trauma, they’re probably going to have long-standing disability from the traumatic head injury,” he said in a September 2025 interview.
The law also reclassifies machines exceeding 28 mph as e-motorcycles, subject to licensing, registration, and insurance. California imposes comparable rules, while New Jersey now goes further, requiring helmets for e-bike riders of every age.
New Hampshire’s group homes for people with brain injuries and developmental disabilities are getting new legislative scrutiny: Gov. Kelly Ayotte signed House Bill 1763 into law on June 19, 2026, creating a committee to study how these residences are sited, built and maintained statewide, and whether siting disputes push vulnerable residents from needed care.
The panel, which was formed after neighbors in towns like Bow objected to state-backed homes appearing without notice, must report findings by Nov. 1, 2026. Sponsor Rep. Mike Drago said “residents feel blindsided” when facilities open unannounced. Disability advocate Lisa Beaudoin countered that “it is perfectly safe to have people with developmental disabilities in one’s neighborhood.” More so, advocates state that it is needed, as New Hampshire’s estimated 2,000 residents with acquired brain disorders rely on such housing to stay near family and services.
New Hampshire isn’t first to grapple with this tension. California has guaranteed small group homes equal footing with single-family houses since 1978. Connecticut adopted similar zoning-parity protections around 1980, later adding density limits after litigation. New York took a study-first approach in 2025, forming a working group on group-home families – a path New Hampshire now follows, as well.
Nearly one in five incarcerated adolescents have a clinically significant brain injury. Most, however, are never diagnosed. New Jersey lawmakers want to change that.
Assembly bill A5104 (introduced May 18, 2026) and its Senate companion S4112 (introduced May 4, 2026) would establish a Brain Injury Screening and Education Program within the Department of Children and Families, targeting children and specific young adults ages 5 to 21, who are in or at risk of entering the mental-health or juvenile-justice systems. The program would deploy validated screening tools, train judges, educators, law enforcement, and facility staff, and fund public outreach on the link between undiagnosed brain injury and delinquency. As stated in the bill’s text, the goal is to “prevent admissions to psychiatric hospitals and reduce the recidivism rates of juveniles adjudicated delinquent.”
Prime sponsor Assemblyman Sterley Stanley is joined in the Senate by Patrick Diegnan, whose history of support for the brain injury committee includes championing New Jersey’s 2010 student-athlete concussion law and earning the Brain Injury Alliance’s Brady Award for Public Service in 2019. Bipartisan Senate co-sponsors are Angela McKnight and Owen Henry.
As of June 2026, no other state has enacted a comparable statutory youth program, making New Jersey a potential national first.
When a law enforcement officer suffers a catastrophic brain injury in the line of duty, the injury itself can make it nearly impossible to ask for help. Georgia Governor Brian Kemp addressed that cruel reality on May 6, 2026, signing House Bill 1128.
Sponsored by Representative Devan Seabaugh and a stated legislative priority of the Kemp administration, HB 1128 allows for a one-time reopening of the application window for officers who have sustained brain injuries to reapply for these benefits. It also amends Georgia code so that legal guardians are notified of those benefits. The Georgia State Indemnification Fund can pay up to $150,000 for brain damage suffered in the line of duty.
“The Kemp family will always back the blue, and I’m proud to sign legislation today that ensures they are supported throughout their careers of service and into retirement,” Governor Kemp said.
The bill corrects a painful catch-22 in which a brain injury can strip an officer of the very cognitive capacity needed to file a claim before a 24-month deadline expires. HB 1128 creates a special application window from July 1, 2026, to August 1, 2026, for public safety officers who suffered total permanent disability due to brain damage sustained in the line of duty on or before July 1, 2024, and whose capacity to apply was impaired by the injury. Unfortunately, some first responders didn’t previously know that they were eligible, which caused many to miss out on this money.
(Kemp has also championed related causes, as the same day he signed “Rio’s Law,” mandating autism-recognition training for police officers. In 2025, he signed the Dignity and Pay Act, which phased out subminimum wages for workers with disabilities. He also signed the GAME Act, in 2024, establishing a statewide framework to recruit and retain employees with disabilities in state government.)
When Vermont Governor Phil Scott signed H.814 into law on May 18, 2026, it marked a quiet but historic moment: every Vermonter gained a legal right to the privacy of their own mind. For the brain injury community, which is a population that increasingly relies on brain-computer interfaces, AI-powered rehabilitation tools, and wearable neurotechnology, the law provides a crucial layer of protection for some of the most intimate data imaginable.
Formally titled “An act relating to neurological rights and the use of artificial intelligence technology in health and human services,” H.814 takes effect July 1, 2026. The bill legally recognizes what should already be commonsense: every Vermonter has a right to “mental and neural data privacy,” “the freedom of thought,” and protection from “unauthorized access to or manipulation of an individual’s brain activity.” For those with brain injuries who depend on neurotechnology for communication, mobility, or cognitive support, that last phrase is a safeguard for the data generated at the most vulnerable intersection of their lives.
With this bill, Vermont joins Colorado, California, Montana, and Connecticut, though each of which has taken a distinct approach to neurological privacy. Colorado and California moved first in 2024, amending existing consumer privacy statutes to classify neural data as sensitive personal information. Montana went further with a standalone law amending its Genetic Information Privacy Act, requiring robust consent and uniquely prohibiting the storage of neural data in U.S.-sanctioned countries. Connecticut’s 2025 amendment was narrower, covering only the central nervous system. Vermont’s law aligns most closely with Connecticut’s, in that it establishes specific rights, while directing the state’s AI Advisory Council to develop further ethical guidelines, which extends through 2030.
Sponsored by State Representative Brian Cina, a clinical social worker, Vermont’s new legislation, and beyond the aforementioned five states that have similar laws, Massachusetts, Minnesota, Illinois, and New York are currently advancing similar bills. For the brain injury community, the question is no longer whether neurotechnology will be part of care and recovery, as it already is. The question is whether the law will keep pace.
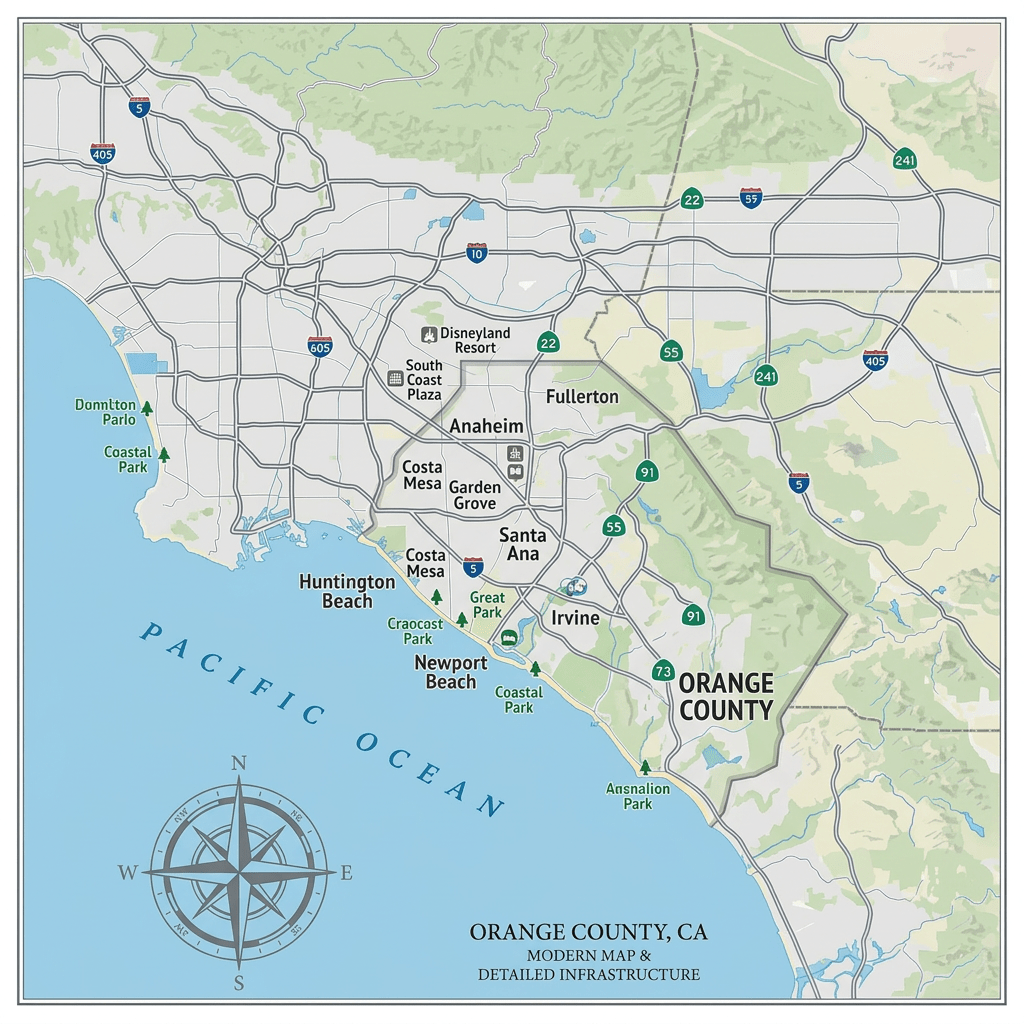
A catastrophic chemical emergency has engulfed Orange County, California, forcing more than 50,000 residents to flee after a massive tank of methyl methacrylate ruptured at the GKN Aerospace facility in Garden Grove. Governor Gavin Newsom declared a state of emergency. President Trump also approved of Newsom’s request for federal aid, unlocking critical FEMA resources to help stabilize the crisis.
What many people don’t realize is that many chemicals, including methyl methacrylate, don’t just threaten the lungs. They also target the brain. Research published on NIH’s PubMed has found that methyl methacrylate causes measurable neurological deficits in exposed industrial workers, impairing memory, learning, and movement. One study documented that vapor exposure depressed electrical activity in the hippocampus, the brain’s memory center. The neurological symptoms of exposure, like headaches, lethargy, and a heavy, numb sensation in the limbs, can take days or weeks to appear.
As research further reveals, chronic exposure can cause degenerative changes in the brain and permanent nerve damage. Children, the elderly, and those with respiratory conditions face the greatest risk. As Garden Grove begins to recover, the invisible injury to thousands of brains is only beginning to unfold.
This concern over industrial chemical dust is not new. California already has the strictest regulations on chemical plants and manufacturers of any state. Proposition 65 states that these companies must provide public warnings if they emit or use hundreds of chemicals linked to cancer or reproductive harm. Beyond just being one of the first states to mandate regulations, New Jersey also imposes some of the most rigorous chemical safety and security standards. Additionally, with the Matt Haller Act, Illinois enforces some of the strictest emission regulations. As Illinois Senator Dick Durbin captured in a 2017 letter addressed to the CDC Director: “It is clear that public exposure to [industrial chemical] dust can lead to serious health, safety, and environmental issues.”
On April 9, 2026, Nebraska’s Legislature passed Legislative Resolution 293 in a 43-0 vote, making it the 14th state – alongside Oklahoma, Texas, Indiana, Kentucky, Arizona, Florida, North Carolina, Wyoming, Maryland, Virginia, North Dakota, Tennessee and Missouri – to formally urge Congress to expand treatment access for veterans suffering from traumatic brain injury and post-traumatic stress disorder, one of the most pressing issues facing American veterans.
Introduced by Nebraska State Senator Kathleen Kauth, the resolution, “[urges] the United States Congress to swiftly enact legislation to provide for veterans’ access to treatments for traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD).”
In particular, states’ resolutions seek to encourage Congress to move forward on hyperbaric oxygen therapy. “A 4-week course of HBOT may alleviate depressive symptoms in PTSD patients, an effect associated with increased serum BDNF and β-NGF levels,” according to a 2026 study, available to view on the NLM database. The United States loses more than 17 veterans per day to suicide, with TBI and PTSD among the leading contributing factors.
Now that 14 states are aligned behind this legislation, the pressure on Congress to act is mounting.
San Antonio Spurs star Victor Wembanyama tumbled face-first on the court in the second quarter of Game 2, on Tuesday, April 21, at the NBA Playoffs against Portland. The accident was both a serious blow to the player and the team, as Wembanyama averages 25.0 points, 11.5 rebounds, and 3.1 blocks per game. Fortunately, he returned for Game 4 of the game series, which San Antonio ultimately won. However, it is a sobering reminder both that nobody is concussion-proof and of the immense importance of NBA’s Concussion Protocol.
Through the years, incidents like Wembanyama’s head trauma have become more common and with greater consequences, as today’s NBA players are stronger and more athletic than those from the past. Due to this situation, the NBA finally had the wherewithal to institute a Concussion Protocol in the 2011–12 season. Before it, reportedly just 5.7 concussions were recorded per season in the League. Afterward, that number nearly tripled, not because the game suddenly got much more dangerous, but because of more “accurate reporting secondary to advances in player education, medical knowledge, national media coverage, and standardized testing protocols,” states a 2019 study, Concussions in the National Basketball Association: An Analysis from 1999-2018, available on PubMed.gov.
“A player diagnosed with a concussion should be regularly monitored for 24 hours … the player may not begin the return-to-participation exertion process until 24 hours after the time of injury,” read the original Protocol. In 2026, the Protocol is more rigorous: a player cannot return to full participation for at least 48 hours and must successfully complete cognitive tests before clearance.
Beyond the pros, college players are at risk, as are basketball players still in high school and younger. In the 2023 – 2024 season, approximately 250,000 students sustained concussions across nine high school sports, according to the National Federation of State High School Associations. Accordingly, Senator Dick Durbin (IL) introduced Protecting Student Athletes from Concussions Act on September 18, 2025. At that time, S.2889 was read twice and referred to the Committee on Health, Education, Labor, and Pensions. On February 17, 2026, Protecting Student Athletes from Concussions Act was introduced to the House by Representative Mark DeSaulnier (CA). H.R.7590 was then referred to the House Committee on Education and Workforce. No action has been taken on either bill since their introductions. (While no federal sports concussion law yet exists, all 50 states have adopted youth sports concussion laws.)
Although injuries do happen, most notably in the NBA, ultimately a player is responsible for their own safety. In August 2024, the government published a systematic review, Sure Steps: Key Strategies for Protecting Basketball Players from Injuries, available on PubMed. Five of the six strategies highlight neuromuscular training, which includes strength work, stabilization or core, mobility, and agility.