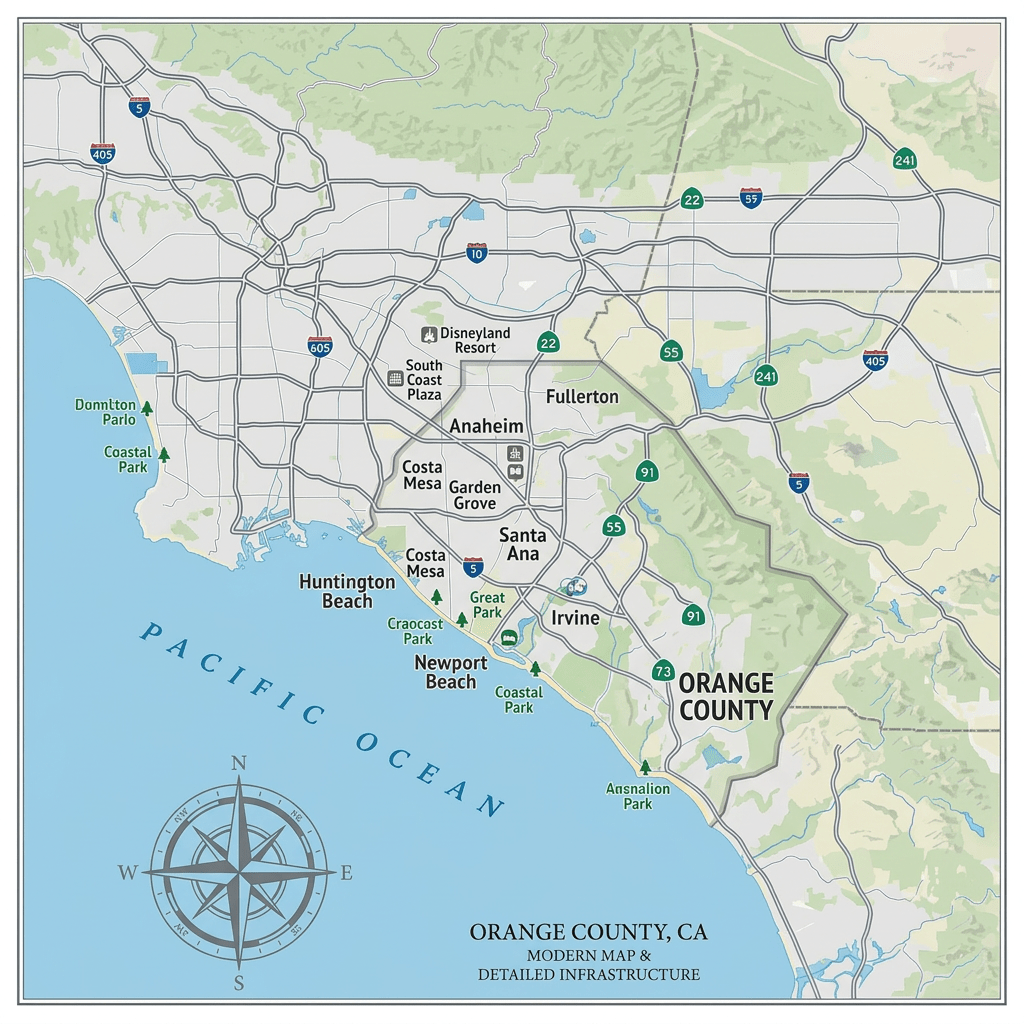
A catastrophic chemical emergency has engulfed Orange County, California, forcing more than 50,000 residents to flee after a massive tank of methyl methacrylate ruptured at the GKN Aerospace facility in Garden Grove. Governor Gavin Newsom declared a state of emergency. President Trump also approved of Newsom’s request for federal aid, unlocking critical FEMA resources to help stabilize the crisis.
What many people don’t realize is that many chemicals, including methyl methacrylate, don’t just threaten the lungs. They also target the brain. Research published on NIH’s PubMed has found that methyl methacrylate causes measurable neurological deficits in exposed industrial workers, impairing memory, learning, and movement. One study documented that vapor exposure depressed electrical activity in the hippocampus, the brain’s memory center. The neurological symptoms of exposure, like headaches, lethargy, and a heavy, numb sensation in the limbs, can take days or weeks to appear.
As research further reveals, chronic exposure can cause degenerative changes in the brain and permanent nerve damage. Children, the elderly, and those with respiratory conditions face the greatest risk. As Garden Grove begins to recover, the invisible injury to thousands of brains is only beginning to unfold.

This concern over industrial chemical dust is not new. California already has the strictest regulations on chemical plants and manufacturers of any state. Proposition 65 states that these companies must provide public warnings if they emit or use hundreds of chemicals linked to cancer or reproductive harm. Beyond just being one of the first states to mandate regulations, New Jersey also imposes some of the most rigorous chemical safety and security standards. Additionally, with the Matt Haller Act, Illinois enforces some of the strictest emission regulations. As Illinois Senator Dick Durbin captured in a 2017 letter addressed to the CDC Director: “It is clear that public exposure to [industrial chemical] dust can lead to serious health, safety, and environmental issues.”